Nerve Entrapment syndromes
A nerve is called entrapped when it losses its mobility and flexibility because of compression by the surrounding tissues.
Causes of Nerve compression syndrome
- Repetitive movement related injuries
- Sprains and fractures following trauma
- Diabetes Mellitus
- Autoimmune disorders like Rheumatoid arthritis
- Thyroid dysfunction
- High blood pressure
- Tumours and cysts
- Obesity
Patho-physiology of Nerve Compression syndrome
Because of the Nerve entrapment, the blood flow to the nerves is reduced which causes swelling in the nerves. This further causes damage to the Myelin sheath layer of the nerves which is responsible for insulation and effective signal transmission. Thus this demyelinating process greatly impacts the nerves ability to send and receive signals which produces symptoms like tingling, numbness and pain.
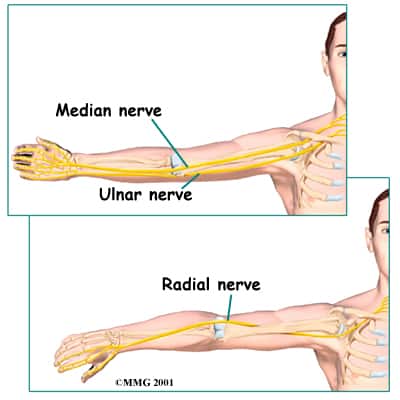
The most common nerves in the upper limb which are responsible for causing Entrapment syndrome and Elbow and wrist pain are:
- Radial nerve
- Median nerve
- Ulnar nerve
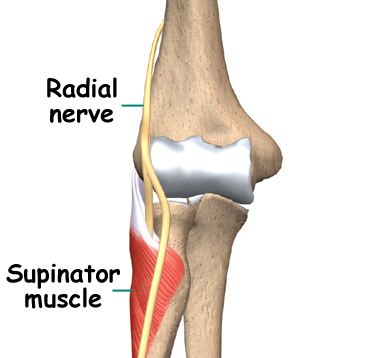
Radial Nerve
Radial nerve is one of the branches of the posterior cord of the brachial plexus and can get entrapped anywhere along its course. Two most common locations are
- Posterior Interosseous nerve syndrome: Posterior interosseous nerve syndrome is a neuropathic compression of the posterior interosseous nerve where it passes through the radial tunnel underneath a musculotendinous arch, the arcade of Frohse. This nerve is the deep motor branch of the Radial nerve which supplies the majority of the forearm and hand extensors and thus produces no sensory deficits.
- Wartenberg syndrome: Entrapment of the superficial branch of the radial nerve with only sensory manifestations and no motor deficits. In this condition, the patient reports pain over the distal radial forearm associated with paresthesia over the dorsal radial hand.
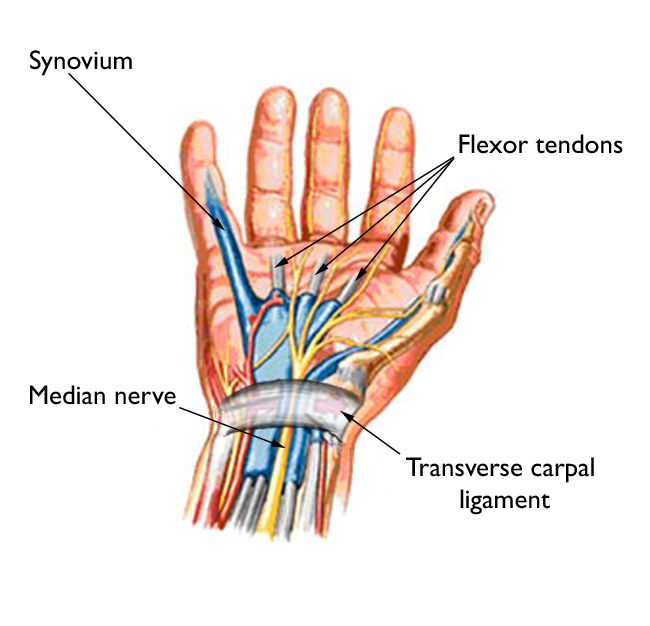
Median nerve
Median nerve is also called as the ‘Eye of the hand’. Forms of median nerve entrapment include the following:
- Carpal tunnel syndrome (CTS): It is the most common form of compression mononeuropathy and caused by compression of the median nerve at the wrist below the Flexor retinaculum.
- Pronator syndrome (or pronator teres syndrome [PTS]): It is defined as compression of the median nerve in the forearm, that results in predominantly sensory alteration in the median nerve distribution of the hand and the palmar cutaneous distribution of the thenar eminence
- Anterior interosseus nerve (AIN) syndrome (AINS): It is characterized by complete or partial loss of motor function of the muscles innervated by the AIN, a motor branch of the median nerve in the forearm.
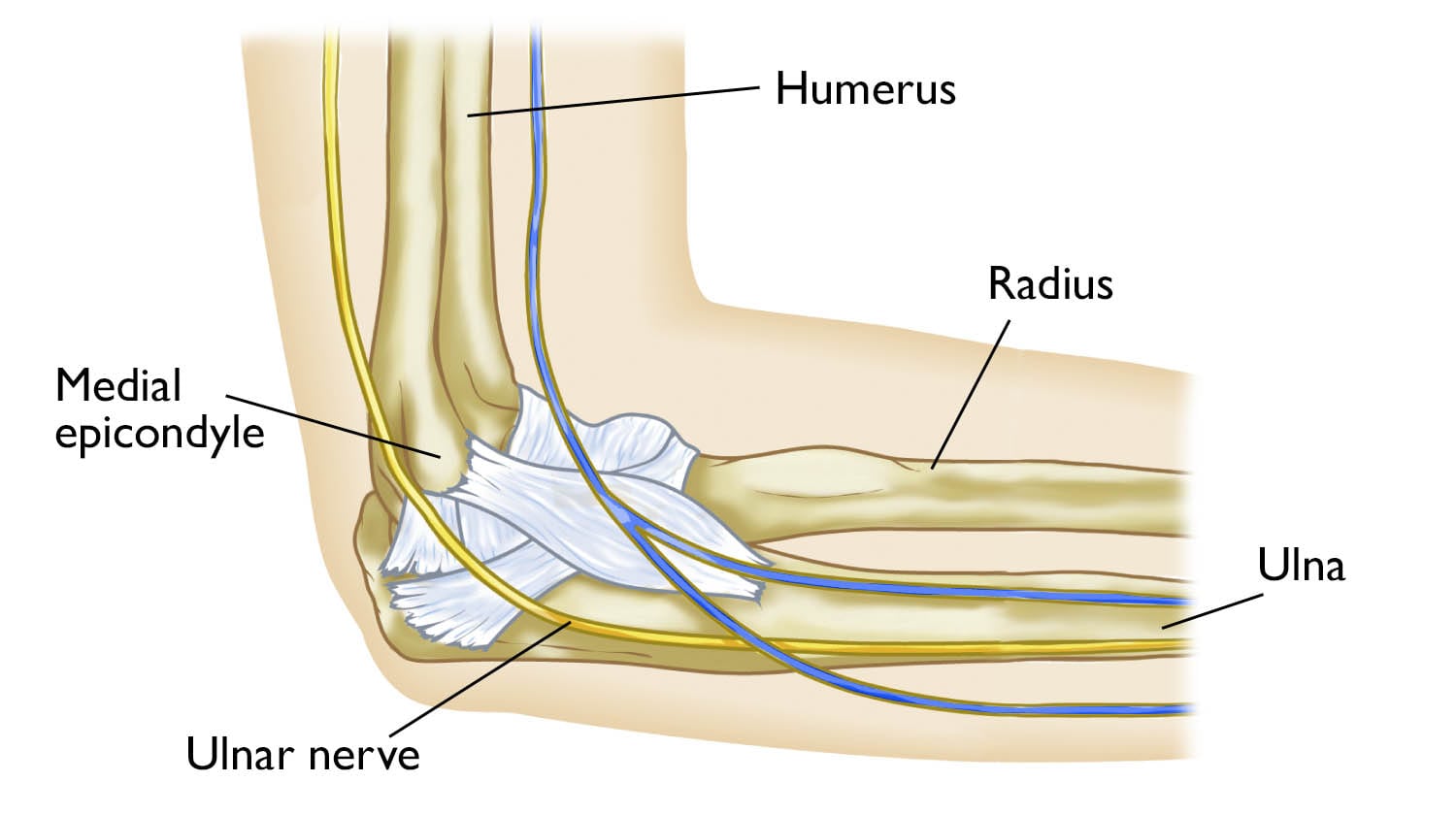
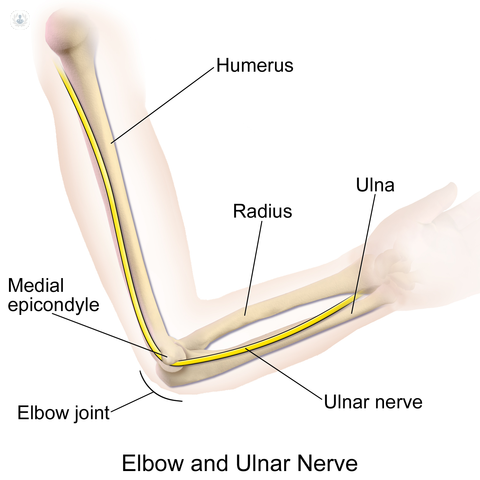
Ulnar nerve
Ulnar nerve is also called as the Musicians nerve as it controls the finger movements. Forms of Ulnar nerve entrapment include the following:
- Cubital tunnel syndrome: It is the second most common form of compression mononeuropathy after carpal tunnel syndrome and is caused by compression of ulnar nerve in the cubital tunnel (a tunnel of muscle, ligament, and bone) situated at the inner aspect of elbow. Patients may present with tingling in fingers 4 and 5, weak grip strength, painand sensitivity on the ulnar side of the forearm, wrist and hand, muscle atrophy, clawing of digits 4 and 5
- Guyon’s canal syndrome: Also called as the Cyclist’s palsy, it occurs when the ulnar nerve becomes entrapped between the hook of the hamate and the transverse carpal ligament due to repetitive compression, from leaning on the elbows or wrists as in the cyclist’s. Patients may present with tingling in fingers 4 and 5, weak grip strength, painand sensitivity on the ulnar side of the hand, muscle atrophy mainly hypothenar, clawing of digits 4 and 5
JEEVISHA protocol for management of Nerve entrapment syndrome
Patients presenting to us with symptoms of nerve entrapment syndrome are first evaluated extensively to determine the cause of the compression i.e. structural or medical. This is done by Clinical examination and Ultrasound examination of the nerve at our centre itself. Some patients may require advanced tests like Nerve conduction studies and MRI neurography.
Targeted treatment
- Ultrasound guided Nerve hydrodissection
- Ultrasound guided Dextrose Prolotherapy